|
About Birth
TACTILE AND
EMOTIONAL SUPPORT DURING LABOR: THE DOULA
Johnson
& Johnson
Photos courtesy of Charis Doulas

"Doula"
is a Greek word meaning "a woman who helps other women." In the
realm of contemporary perinatal care, the term has come to mean a
caregiver who provides continuous physical, emotional and
educational support to the mother before, during and just after
childbirth. Doulas stay with the mother throughout labor, constantly
assessing and responding to her needs.

A doula is a layperson, most often a woman, who understands the
biological and medical processes involved in labor and obstetrics,
and who usually has assisted in at least five or six deliveries
under the supervision of another doula. Her training also provides
her with knowledge of obstetrical interventions, so that she can
explain them to the woman and her partner in the event they are
needed.
Doulas typically function as a part of the "birthing team," serving
as an adjunct to the midwife or the hospital obstetrical staff. Physicians and labor and delivery nurses may appreciate the doula's
sustained attention to the mother, especially in hospitals where
demands on the staff interfere with exclusive contact with the
mother. The doula also serves a critical role in supporting and
educating the woman's partner, enabling him or her to be as involved
and as effective as possible in supporting the mother.
In the United States, most doulas work as independent providers
hired by the expectant woman. (In fact, many hold full-time jobs
outside the realm of health care.) Increasingly, managed care
organizations are offering doula support as part of regular
obstetrical care. In some European institutions, doula support is
offered as a standard of care by midwives or nursing students. In many cultures, of
course, the practice of a knowledgeable woman helping a mother in
labor is not labeled anything as official as "doula" support; it is
simply an ingrained, centuries-old custom.
Overall, the defining characteristic of doula-type care is
continuous, uninterrupted, emotional and physical support of the
woman for the duration of the labor and childbirth. -21
THE ROLE OF TOUCH IN
DOULA CARE
 The doula can use many kinds of touch and massage, depending on what
the mother finds helpful. Doulas may, for example, gently touch or
stroke the mother's shoulder, hand or foot while offering
reassurance. They regularly confirm what type of touch and body
positions the mother is finding most beneficial, and alter their
touch as needed. The doula can use many kinds of touch and massage, depending on what
the mother finds helpful. Doulas may, for example, gently touch or
stroke the mother's shoulder, hand or foot while offering
reassurance. They regularly confirm what type of touch and body
positions the mother is finding most beneficial, and alter their
touch as needed.
As labor progresses, the doula may cradle the woman in her arms,
wipe her brow, massage her and use other forms of touch as she
educates her about what is happening to her body and in the birth of
her child. She often instructs the partner or birth companion in
doing the same, helping him or her to soothe the mother. Together,
the doula and the partner may physically support the laboring mother
in walking, sitting, leaning or squatting. To relieve back labor,
the doula might use back rubs, hot cloths and pressure.
Studies have documented that a doula's touch and support leads to
reduced pain-or, at the very least, the mother's perception of
reduced pain. Controlled comparisons of women who received doula
support with those who did not revealed that mothers in the "doula
groups" reported significantly less labor pain. 22
The doula provides support after birth as well. Among other things,
she may facilitate the parents' bonding with the child by
encouraging close contact from the moment of birth, especially in
the first hour.
CLINICAL BENEFITS OF
DOULA SUPPORT
 Within the past decade, a number of controlled studies have
supported the use of doulas. Among these studies, two conducted in
Guatemala City and one in Houston, Texas are of particular
interest. -23, -24, -25 In all three, the investigators randomly assigned
first-time mothers to doula support or no doula support. In
comparisons between the doula and no-doula groups, the data were
adjusted for interventions such as oxytocin and C-sections, making
the presence or absence of a doula the only major difference in the
labor environments of these two groups. Within the past decade, a number of controlled studies have
supported the use of doulas. Among these studies, two conducted in
Guatemala City and one in Houston, Texas are of particular
interest. -23, -24, -25 In all three, the investigators randomly assigned
first-time mothers to doula support or no doula support. In
comparisons between the doula and no-doula groups, the data were
adjusted for interventions such as oxytocin and C-sections, making
the presence or absence of a doula the only major difference in the
labor environments of these two groups.
PICTURE
The defining characteristic of doula care is continuous,
uninterrupted emotional and physical support of the woman throughout
labor and childbirth.
Data from those studies, which demonstrate the benefits of doula
support, are described below and summarized in Table 1 -22
Length of Labor. The studies showed that doula support
reduced labor time. Researchers were able to conclude that in spite
of obstetrical methods of inducing and speeding up labor (e.g.,
artificial rupture of membranes, augmentation of contractions, forcep deliveries, C-sections), the mothers who received doula
support were the ones with the shortest labors.
Vaginal Deliveries vs. C-sections. By conservative estimates,
cesarean sections are performed in about 20 to 25 percent of U.S.
births each year. In contrast, C-section rates among doula-assisted
groups in these studies were lower: seven to eight percent.
Table 1.
Need for interventions in births without and with doulas -22
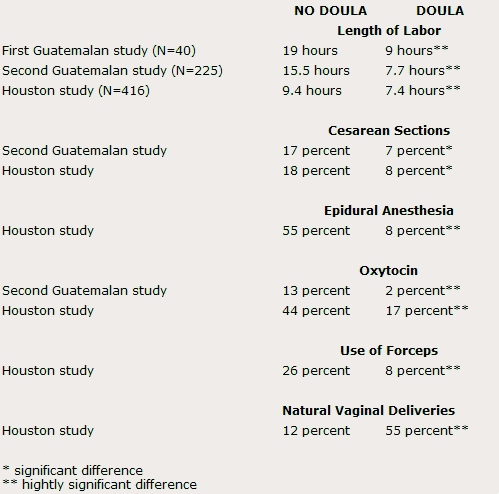
Epidural Anesthesia. In the Houston study, more than half of
the women without a doula requested or required epidural
anesthesia-compared with only eight percent in the doula group.
Oxytocin. In one Guatemalan study, only two percent of women
who had a doula required oxytocin, a drug that increases the
strength of contractions; 13 percent in the control group needed the
drug. The Houston study documented significantly larger percentages
in both groups. While oxytocin is helpful to some mothers, it causes
contractions to become more forceful and painful-leading some women
to need an epidural or other pain medication as a result of the
oxytocin's effects.
Forceps. Although physicians use forceps much less often
today than in the past two decades, this tool is still helpful in
some deliveries, especially when epidurals have been administered.
The studies document forceps deliveries eight percent for
doula-supported births, compared with 26 percent in the control
group, a difference largely due to the more frequent use of epidural
anesthesia in the no-doula groups.
Natural Deliveries. In the Houston study, 55 percent of the
doula-supported women had natural vaginal deliveries-that is,
delivery without C-section, anesthesia, oxytocin, medication or
forceps-whereas only 12 percent of the women without doulas
delivered naturally. In the words of the authors, "it is fascinating
to reflect that the presence of one caring woman throughout labor
resulted in such a large difference." -22
INSTITUTIONALIZED USE
OF DOULAS: A CLINICAL MODEL

About 25 years ago, the National Maternity Hospital in Dublin,
Ireland, introduced continuous emotional support on its labor and
delivery units, in addition to a strict definition of the onset of
labor. The results were impressive and so beneficial that the
hospital established doula-type care - delivered by nurse-midwifery
students - as a mainstay of its maternity services for all patients. Key results of this labor-support program include:
1. a
drop in the hospital's average length of labor to between a half to
a third of what it had been before the program. Since the late
1980s, the mean length of labor for first-time mothers at the
hospital has been slightly less than six hours. (The program also
uses membrane rupture and oxytocin to assure a certain dilation
rate.);
2. a C-section rate of five to six percent that has been sustained
for two decades; -22 and
3. a significantly increased patient census, facilitated in large
part by the shorter labors, lack of complications and more rapid
patient discharge following most of the births. -21
BEYOND LABOR: BENEFITS
TO MOTHER AND BABY AFTER BIRTH

The benefits of doula support do not end in the delivery room.
Rather, benefits have been evident in both mother and infants long
after the birth and the doula's support.
Mothers' first 24 hours. In the Guatemalan study, the
researchers observed the women in the doula and no-doula groups
through a one-way mirror for the first 25 minutes after the mothers
left the delivery rooms. The ratings showed that the doula-supported
mothers had more affectionate interaction with their infants,
smiling, stroking and talking to their newborns more than did the
no-doula mothers. -22
In addition, studies in Johannesburg, South Africa looked at 189
first-time mothers who had an untrained laywoman supporting them
throughout labor. These female caregivers constantly used touch and
verbal encouragement to comfort and reassure the women. -26, -27
The new mothers who received doula care:
1. reported less pain during childbirth at the one-day postpartum
interview than they expected, while the control group mothers
reported more discomfort; and
2. reported less anxiety at 24 hours and 6 weeks postpartum (even
though the groups had similar levels of anxiety before labor), had a
better perception of how they had coped with the birth experience,
and spent more time with their babies after birth.
The newborn at six weeks. Positive effects of doula support
on the infant were also evident weeks after the doula's involvement
was over.
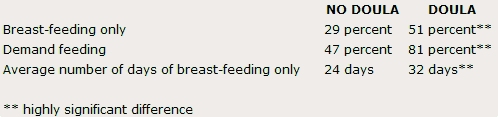
Infant feeding. In the Johannesburg study, the doula-supported group
showed a significantly higher incidence of breast-feeding and
"on-demand" feeding. Also, 63 percent of the no-doula group
experienced feeding problems with the newborn, while only 16 percent
of the doula group experienced problems. -22
Table 2.
Feeding behavior at six weeks with and without doulas - 22
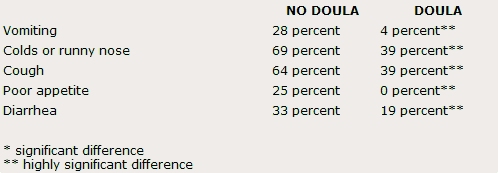
Infant health. Although the infants had been similar in
all respects at birth, mothers in the two groups from the
Johannesburg study reported marked differences in the health of
their babies at six weeks. The research did not determine whether
these were perceptual or actual differences, but doula care during
labor and delivery clearly instilled some attitudinal or physical
advantages to mother or child, or both. Some of the differences may
be related to the higher incidence of breast-feeding in the doula
group.22
Table 3.
Infant health problems at six weeks after birth with and without
doulas - 22
Mother-infant bonding. Mothers in the doula group reported
spending 1.7 hours a week away from their babies, as opposed to 6.6
hours reported by the no-doula group. The doula-group mothers
reported an average of 2.9 days to develop a relationship with the
baby, compared to 9.8 days for the other group of mothers. The
results suggest that mothers in the doula group were more available
and better able to form an attachment with their newborns. -22
Mothers' emotional state. Psychological tests in the
Johannesburg study found significantly less anxiety, fewer signs of
depression and a higher level of self-esteem in the doula-group
mothers, suggesting that, among other things, they are less likely
to suffer postpartum depression. Mothers who feel better about
themselves are also more likely to provide a nurturing environment
for their infants.
Researchers also reported that doula-supported mothers felt a great
increase in satisfaction with their partner after the birth of the
baby. Mothers who did not receive doula support did not express this
degree of satisfaction. In a variety of areas, the doula-supported
mothers' perceptions of themselves, their babies and their partners
were clearly more favorable. -22
MECHANISM OF ACTION:
WHY DOES DOULA SUPPORT WORK?

The mechanism of action by which doula care produces its positive
effects is unknown but is assumed to involve the combined influences
of the doula's physical and psychological interventions.
Some investigators theorize that the catecholamine stress hormones
adrenalin and noradrenalin cause the labor of many mothers to slow
down, making complications more likely and the labor experience more
taxing and stressful. By calming the patient through touch,
reassurance and relaxation, however, the doula may alleviate the
woman's fear and apprehension and, in turn, help to moderate the
hormonally mediated stress reactions, ultimately lessening the need
for medical intervention and shortening the labor.
IMPLICATIONS FOR
HEALTHCARE COSTS
When Klaus et al. conducted a meta-analysis of six randomized doula
studies, they reached the conclusion that the presence of a doula
reduces the overall cesarean rate by 50 percent, length of labor by
25 percent, oxytocin use by 40 percent, pain medication by 30
percent, the need for forceps by 40 percent, and request for
epidurals by 60 percent.
These results indicate the potential financial benefits of doula
services, on both institutional and national levels. If widespread
use of doula services were to cut the number of cesarean sections in
the U.S. by half and reduce epidural use as well, savings in the
nation's medical-care costs would be an estimated $1.3-1.6 billion
annually. -21
REFERENCE
1.
Spitz RA. Anaclitic depression. Psychoanalytic Study of the
Child.1946;2:313-347.
2.
Suomi SJ, Brown CC et al. The role of touch in rhesus monkey social
development. In The Many Facets of Touch, Johnson & Johnson
Pediatric Roundtable. 1984;10:41-56.
3.
Suomi SJ. Interview, 1994.
4.
Seay BM, Harlow HF. Maternal separation in the rhesus monkey.
Journal of Nervous and Mental Diseases. 1965;140:434-441.
5.
Seay BM, Hansen EW, and Harlow HE Mother-infant separation in
monkeys. J. Child Psychol. Psychiatry. 1962;3:123-132.
6.
Bowlby J. Attachment. New York: Basic Books; 1969.
7.
Harlow HE The heterosexual affectional system in monkeys. American
Psychologist. 1962b;17:1-9.
8.
Goy RW, Wallen K, and Goldfoot DA. Social factors affecting the
development of mounting behavior in male rhesus monkeys. In
Reproductive Behavior, Montagna W and Sadler W, eds. New York:
Plenum Press; 1974.
9.
Suomi SJ. Genetic and maternal contributions to individual
differences in rhesus monkey biobehavioral development. In Perinatal
Development: A Psychobiological Perspective, Krasnegor N et al.,
eds. New York: Academic Press; 1987:397-420.
10.
Fairbanks LA. Early experience and cross-generational continuity of
mother-infant contact in vervet monkeys. Developmental
Psychobiology. 1989;27:669-681.
11.
Suomi SJ. Primate separation models of affective disorders. In
Neurobiology of Learning, Emotion and Affect, Madden H, ed. New
York: Raven Press, Ltd.; 1991 :195-214.
12.
Schanberg S, and Field T. Maternal deprivation and supplemental
stimulation. In Stress and Coping Across Development, Field T,
McCabe P, and Schneiderman N, eds. Hillsdale, NJ: Erlbaum; 1988.
13.
Higley JD, Suomi SJ, and Linnoila M. A longitudinal assessment of
CSF monoamine metabolite and plasma cortisol concentrations in young
rhesus monkeys. Biological Psychiatry. 1992;32:127-145.
14.
Schanberg S et al. Maternal deprivation and growth suppression. In
Advances in Touch, Johnson & Johnson Pediatric Roundtable,
Gunzenhauser N, ed. 1989;14:3-10.
15.
Meaney MJ, Aitken DH, Bodnoff SR, Iny U, and Sapolsky RM. The effect
of postnatal handling on the development of the glucocorticoid
receptor systems and stress recovery in the rat. Progress in
Neuropsychopharmacology and Biological Psychiatry. 1985;7:731-734.
16.
Reite M. Effects of touch on the immune system. In Advances in
Touch, Johnson & Johnson Pediatric Roundtable, Gunzenhauser N, ed.
1989;14:22-31.
17.
Laudenslager M, Reite M, and Held P. Early mother-infant separation
experiences impair the primary but not the secondary antibody
response to a novel antigen in young pigtail monkeys. Psychosomatic
Medicine. 1986;48:304.
18.
Coe CL, Lubach G, Ershler WB, and Klopp RG. Influence of early
rearing on lymphocyte proliferation response in juvenile monkeys.
Brain, Behavior, and Immunity. 1989;3:47-60.
19.
Laudenslager ML, Rasmussen KLR, Berman CM, Suomi SJ, and Berger CB.
Specific antibody levels in free-ranging rhesus monkeys:
relationships to plasma hormones, cardiac parameters, and early
behavior. Developmental Psychology. 1993;26:407-420.
20.
Suomi SJ. Touch and the immune system in rhesus monkeys. In Touch in
Early Development, Field TM, ed. Hillsdale, NJ: Lawrence Erlbaum
Assoc.; (in press).
21.
Klaus MH. Interview, 1994.
22.
Klaus MH, Kennell, JH and Klaus, PH. Mothering the Mother. Reading,
Massachusetts: Addison-Wesley Publishing Company; 1993.
23.
Sosa R, Kennell JH, Robertson S, and Urrutia J. The effect of a
supportive companion on perinatal problems, length of labor and
mother-infant interaction. New England Journal of Medicine.
1980;303:597-600.
24.
Klaus MH, Kennell JH, Robertson SS, and Sosa R. Effects of social
support during parturition on maternal and infant morbidity. BMJ.
1986;293:585-587.
25.
Kennell JH, Klaus MH, McGrath SK, Robertson SS, and Hinkley CW.
Continuous emotional support during labor in a U.S. hospital.
Journal of the American Medical Association. 1991;265:2197-2201.
26.
Hofmeyer GJ, Nikodem VC, and Wolman WL. Companionship to modify the
clinical birth environment: effects on progress and perceptions of
labour and breast feeding. British Journal of Obstetrics and
Gynecology. 1991;98:756-764.
27.
Wolman WL. Social support during childbirth: psychological and
physiological outcomes. Masters' thesis. University of
Witwatersrand, Johannesburg; 1991.
28.
Field TM, et al. Tactile/kinesthetic stimulation effects on preterm
neonates. Pediatrics. 1986;77:654-658.
29.
Acolet D, et al. Changes in plasma cortisol and catecholamine
concentrations in response to massage in preterm infants. Archives
of Disease in Childhood. 1993;68:29-31.
30.
Solkoff N and Matuszak D. Tactile stimulation and behavioral
development among low-birthweight infants. Child Psychiatry and
Human Development. 1975;6:33-37.
31.
White J and Labarba R. The effects of tactile and kinesthetic
stimulation on neonatal development in the premature infant.
Developmental Psychobiology. 1976;6:569-577.
32.
Ottenbacher KJ, Muller L, Brandt D, Heintzelman A, Hojem P. and
Sharpe P. The effectiveness of tactile stimulation as a form of
early intervention: a quantitative evaluation. Journal of
Developmental and Behavioral Pediatrics. 1987;8:68-76.
33.
Field TM. Interview, 1994.
34.
Field TM, et al. Massage therapy for infants of depressed mothers.
Miami, Florida: Touch Research Institute, University of Miami School
of Medicine; 1994.
35.
Klaus MH and Klaus PH. The Amazing Newborn. Reading, Massachusetts:
Addison-Wesley Publishing Company; 1985.
36.
Kuhn C, Schanberg S, Field T, Symanski R, Zimmerman E, Soafidi F,
and Roberts J. Tactile/kinesthetic stimulation effects on
sympathetic and adrenocortical function in preterm infants. Journal
of Pediatrics. 1991;119:434-440.
37.
Current Touch Research Institute Studies (listing available from
Touch Research Institute, University of Miami School of Medicine).
38.
Preliminary data: TRI Massage Studies (information available from
Touch Research Institute, University of Miami School of Medicine).
39.
Lester BM, Boukydis CFZ, Garcia-Coil CT, and Hole WT. Colic for
developmentalists. Infant Mental Health Journal. 1990;11:4,321-333.
40.
Liepack S, et al. Infant colic: a review. (Unpublished manuscript.)
Miami, Florida: Touch Research Institute, University of Miami School
of Medicine.
41.
Massage effects on asthmatic children. (Unpublished manuscript.)
Miami, Florida: Touch Research Institute, University of Miami School
of Medicine.
42.
Wheeden A, et al. Massage effects on cocaine-exposed preterm
neonates. Journal of Developmental and Behavioral Pediatrics.
1994:14, 318-322.
43.
Field TM. Infant massage. In Zero to Three. Bulletin of the National
Center for Clinical Infant Programs; 1993;14(2):8-12.
44.
Field TM, et al. Massage reduces anxiety in child and adolescent
psychiatric patients. J. Am Acad. Child Adolesc. Psychiatry. 1992;31
(1):125-131.
45.
Scholz K, Samuels C. Neonatal bathing and massage intervention with
fathers, behavioral effects 12 weeks after birth of the first baby:
The Sunraysia Australia Intervention Project. Int'l. J. of Behavior
Development. 1992;1~5:67-81.
46.
Righard L, Alade MO. Effects of delivery room routines on success of
first breast-feed. Lancet. 1990;77(5):1105-1107.
47.
Klaus MH, Kennell JH et al. Human maternal behavior at the first
contact with her young. Pediatrics. 1970;46:187-192.
48.
Kaitz M, Lapidot P, Bonner R, and Eidelman A. Parturient women can
recognize their infants by touch. Developmental Psychology.
1992;28:35-39.
49.
Kaitz M, et al. Fathers can also recognize their infants by touch.
(Unpublished manuscript.) Hebrew University of Jerusalem, Department
of Psychology; 1992.
This
monograph for healthcare professionals is provided to you by
Johnson & Johnson
Touch In Labor and Infancy

'Behold, I will bring them from the north country, And gather them
from the ends of the earth,
Among them the blind and the lame,
The woman with child and The one who labors with child, together,
A
great throng shall return there...And My people shall be satisfied with My goodness, says the LORD.'
Jeremiah 31:8, 14~~~
©2009 Charis Childbirth
Services, All Rights Reserved
Feel free to forward this newsletter to friends in its entirety,
leaving all attribution intact.
May 2010
|
